IV Therapy for Postural Orthostatic Tachycardia Syndrome (POTS)
Rapid Volume Expansion for Medication-Refractory POTS
Schedule a ConsultationUnderstanding IV Therapy for POTS
IV therapy can provide rapid, short-term symptom relief in many people with POTS by expanding intravascular volume, but evidence is limited, protocols vary, and long-term benefit and safety remain uncertain. At CarePoint Infusion Center, we provide carefully managed IV saline therapy for select patients with medication-refractory Postural Orthostatic Tachycardia Syndrome throughout Cleveland, Beachwood, Westlake, Hudson, Akron, and Northeast Ohio.
Important Note
IV therapy for POTS is not a first-line treatment. It is reserved for patients who have failed optimized conservative management including oral hydration, salt supplementation, compression garments, exercise, and pharmacologic therapy. This intervention should be managed by experienced clinicians with careful patient selection and ongoing monitoring.
What is Postural Orthostatic Tachycardia Syndrome (POTS)?
Postural Orthostatic Tachycardia Syndrome (POTS) is a disorder of orthostatic intolerance characterized by excessive heart rate increase on standing (≥30 bpm in adults, ≥40 bpm in adolescents) and multisystem symptoms including lightheadedness, palpitations, fatigue, brain fog, and exercise intolerance. Volume depletion or low plasma volume is a common contributor to symptoms, which is why fluid and salt loading are first-line measures in management.
How IV Therapy Works for POTS
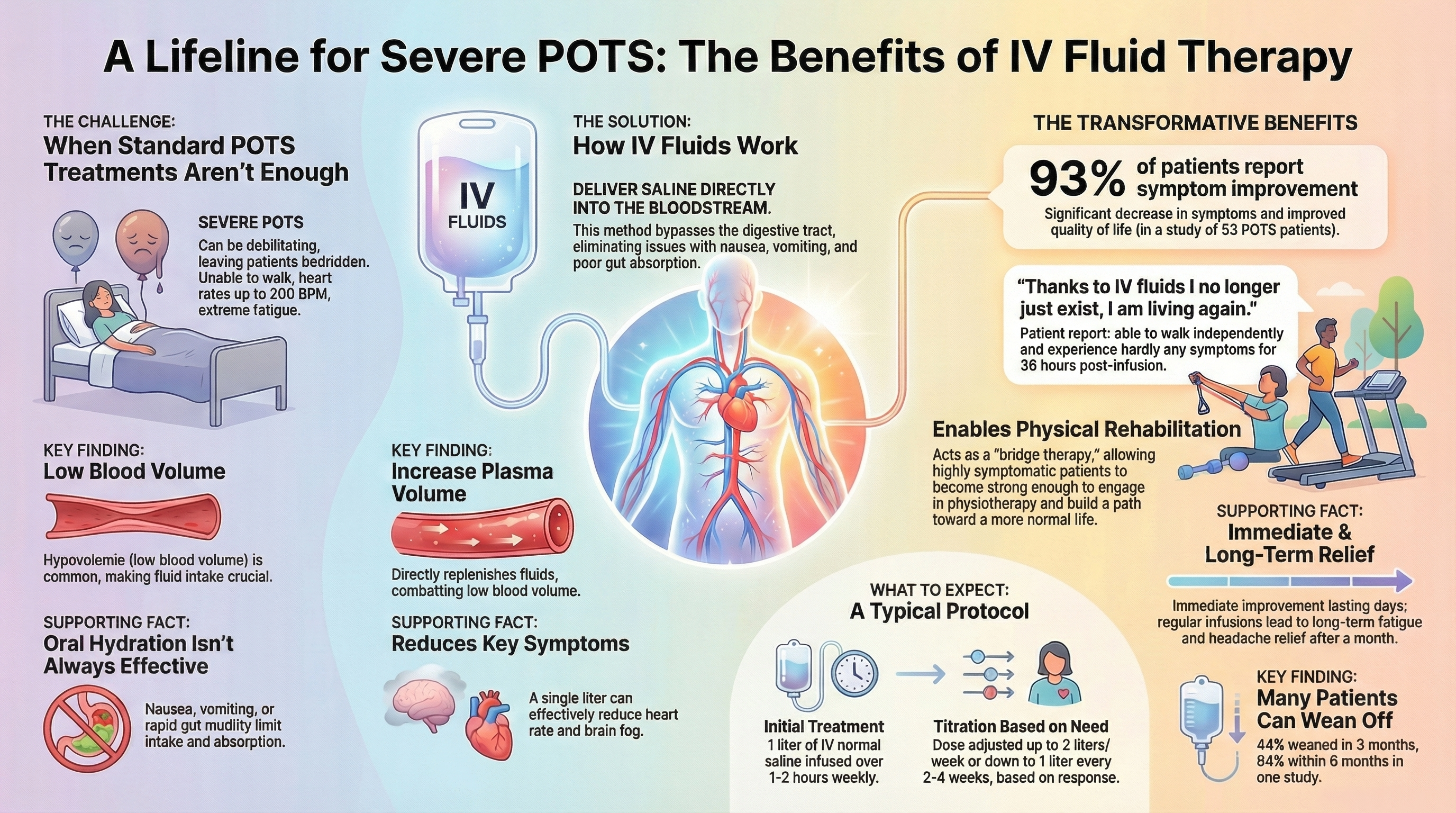
IV saline delivers fluid and electrolytes directly into the bloodstream, rapidly increasing plasma volume, improving venous return, and reducing orthostatic tachycardia and cerebral hypoperfusion. This bypasses gastrointestinal absorption limits and can produce symptom relief within hours to days in responsive patients.
Key Benefits of IV Therapy for POTS
Rapid Symptom Relief
IV saline provides immediate volume expansion, with patients often reporting improvement in lightheadedness, brain fog, and energy levels during and after infusion. Symptom relief typically begins within hours.
Hemodynamic Improvement
Studies demonstrate measurable reductions in standing heart rate and improvements in orthostatic tolerance following saline infusion. The hemodynamic effects typically last 24-72 hours.
Bypasses GI Limitations
Direct intravascular delivery circumvents absorption issues common in POTS patients, including gastroparesis, rapid motility, and nausea that limit oral intake.
High Efficacy Rates
Clinical studies report that 79-93% of medication-refractory POTS patients experience significant symptom improvement with intermittent IV saline infusions.
Bridge to Recovery
IV therapy can serve as a temporary bridge intervention, providing stability to allow patients to implement exercise programs and other long-term strategies. Studies show 94% of patients successfully wean off IV therapy within 6 months.
Improved Quality of Life
For severely affected individuals, regular infusions can restore the ability to perform activities of daily living, engage in social activities, and participate in physical therapy.
of medication-refractory POTS patients report significant symptom improvement with intermittent IV saline infusions (Ruzieh et al., 2017)
Clinical Evidence and Efficacy
Symptom Improvement Rates
Multiple studies demonstrate substantial benefit from intermittent IV saline therapy:
Research Reference
Ruzieh et al. (2017): A landmark study of 53 patients with medication-refractory POTS found that 93% of patients reported significant symptom improvement with intermittent saline infusions, with Orthostatic Hypotension Questionnaire (OHQ) scores improving by 3.1 points, representing clinically meaningful relief. Long-term follow-up data showed 44% of patients weaned off IV therapy within three months, and 94% within six months, suggesting IV therapy serves effectively as a bridge intervention.
Physiological Parameters
Acute volume loading demonstrates measurable hemodynamic improvements:
- Rapid infusion of 1L normal saline over one hour produces dramatic decreases in standing heart rate compared to placebo, midodrine, and clonidine
- The hemodynamic effects typically last 24-72 hours, with symptomatic relief persisting 3-7 days on average
- Peak benefit occurs within minutes to hours after infusion, providing a therapeutic window for patients to engage in daily activities
Treatment Protocols and Patient Selection
Standard Infusion Parameters
Common pragmatic approaches used in clinics include:
| Parameter | Typical Range | Most Common |
|---|---|---|
| Volume | 1-2 liters | 1.5 liters |
| Infusion Rate | 1-2 hours | 1.5 hours |
| Frequency | Every 7-14 days | Every 11 days (average) |
| Solution | Normal saline (0.9% NaCl) | 0.9% Sodium chloride |
Appropriate Candidates
IV saline therapy is indicated for POTS patients who:
- Have persistent symptoms despite optimized oral hydration (2-3L daily) and salt intake (8-10g daily)
- Experience gastrointestinal limitations preventing adequate oral volume intake (gastroparesis, severe nausea/vomiting)
- Require bridge therapy during implementation of exercise programs or other long-term interventions
- Experience acute decompensation during illness, pregnancy, or pre/post-surgical periods
Treatment Course and Weaning
IV therapy should be viewed as a bridge strategy rather than lifelong dependency:
- Initial phase: Weekly infusions for 2-4 weeks to establish symptom control
- Titration: Gradual interval extension based on symptom recurrence patterns
- Weaning: As patients improve, 44% discontinue within 3 months and 94% within 6 months
- Reassessment: Clinical evaluation every 3-6 months to determine ongoing necessity
Risks and Monitoring
IV therapy carries risks that must be carefully considered:
Infection Risk
Infection and thrombosis with long-term central lines are serious concerns. Central venous access devices (PICC lines, ports) carry higher infection rates than peripheral IVs. Catheter-related bloodstream infections can be life-threatening.
Fluid Overload
Excessive intravascular volume can strain the heart and lungs, particularly in patients with underlying cardiac or renal disease. Careful monitoring is essential to prevent pulmonary edema.
Electrolyte Disturbances
Large volumes of normal saline can cause hypernatremia and hyperchloremic metabolic acidosis. Periodic laboratory monitoring of electrolytes and kidney function is recommended.
Vascular Access Complications
Repeated peripheral IV access can damage veins over time, eventually requiring central access. Central lines carry risks of thrombosis, migration, and mechanical complications.
Mitigation Strategies
- Use the least invasive access feasible (peripheral IV preferred over central lines when possible)
- Monitor electrolytes and volume status regularly
- Implement strict aseptic technique and infection surveillance protocols
- Reassess benefit regularly to avoid unnecessary chronic access-related risks
- Consider balanced crystalloid solutions (Plasma-Lyte, Lactated Ringer's) to reduce hyperchloremic acidosis risk
Clinical Recommendations
Current consensus positions IV saline therapy as a third-line intervention:
- First-line: Oral hydration (2-3L daily), dietary salt (8-12g sodium), compression garments, exercise
- Second-line: Pharmacologic therapy (beta-blockers, fludrocortisone, midodrine, ivabradine)
- Third-line: IV saline therapy for refractory symptoms or GI limitations
- Adjunctive: Lifestyle modifications, physical therapy, autonomic conditioning
Key Principles
- Start with conservative measures (oral salt, fluids, compression, exercise) and medications before IV therapy
- Reserve IV saline for refractory or acute hypovolemia, and individualize frequency/dose based on response and safety considerations
- Use the least invasive access feasible, monitor electrolytes and volume status, and reassess benefit regularly to avoid unnecessary chronic access-related risks
Serving Northeast Ohio Communities
CarePoint Infusion Center provides expert IV saline therapy for POTS throughout Northeast Ohio. We serve patients from Cleveland, Beachwood, Westlake, Hudson, Akron, and surrounding communities in Cuyahoga County and beyond.
We conveniently serve patients from:
And throughout Cuyahoga County, Summit County, and Northeast Ohio. Contact us today to schedule your consultation.
Ready to Explore IV Therapy for POTS?
If you have medication-refractory POTS and have exhausted conservative management options, IV saline therapy may be an appropriate consideration. Our experienced team provides careful patient evaluation, individualized protocols, and ongoing monitoring to ensure safety and efficacy.
Looking for additional IV therapies? Visit our Infusion Services hub to explore other treatment options, or return to the CarePoint Infusion homepage.
Medical Disclaimer: This information is for educational purposes only and should not replace professional medical advice. Always consult with a qualified healthcare provider for diagnosis and treatment of medical conditions. Individual results may vary. IV therapy for POTS is not a first-line treatment and should only be considered after exhausting conservative management options. This intervention carries significant risks including infection, thrombosis, and vascular complications, particularly with long-term central access devices. Treatment decisions should be made in partnership with experienced healthcare providers based on individual medical circumstances.